We need a holistic reimagining of the entire healthcare system in UK including desired outcomes and policy framework before determining the future role and operating model of the NHS.
Stephen (Steve) Wyatt is the Professor of Leadership at the University of Bath as well as an author and consultant on leadership. His perspective on leadership whilst refined through rigorous research is also informed by his direct personal experiences. Notable in his national policy work has been revitalisation, growth and navigating significant unfolding changes in sectors including HealthCare, Tourism, Retail and Media. His corporate work has mainly focused on transformation to thrive in the dynamic 4th Industrial Revolution and managing international growth and complexity. His two most recent books are available from Amazon.
As the structure of society evolves, expectations change and technologies develop. It is almost impossible to imagine that policy frameworks and operating models designed decades ago can escape being updated. Just because something was fit-for-purpose when it was conceived and initially designed, doesn’t mean that it will always be so. The more people invested in the operations of a system or impacted by its functioning, the greater the diversity of opinions about what updates to bring. Opinions are even more entrenched if the topic triggers a high emotional reaction – and that is where we are with Healthcare in the UK. So much so in fact, that it is almost impossible to have a coherent conversation about reimagining healthcare in UK without a loud chorus of opinions about one component – the NHS.
It is impossible for the NHS to deliver excellent healthcare in the modern context - the policy framework and operating model were not designed for today. Some of the things that have changed dramatically since 80 years ago include:
- Life Expectancy: From approx. 8-10%, to now 23-26% of the population is >60, this age group represent approx. 40% of healthcare costs.
- Medical Advances: New drugs and new treatments - are disproportionately expensive, and a ‘free for all’ approach escalates treatment costs
- Overweight and Obese: In the 1950s (full records don’t exist) but estimates are approx. 22% of men were overweight with approx. 6% obese, whereas now 64% of adults are overweight or obese!
- Healthcare in the UK in 1950s was approx. 3-3.5% GDP. Now its approx. 12%! It’s the biggest single expenditure in the national budget. More than 2x the entire education spending and nearly 6x the entire defence budget.
That successive generations of governments, healthcare providers and leaders of the NHS have failed to reimagine and resolve the quandary of healthcare in UK is neither a surprise, nor is it excusable.
- As a result the costs have spiralled, whilst pressures have been placed on the provider (NHS) to seek efficiencies.
- Wages for front-line staff are intolerably low, causing recruitment and retention problems as well as contributing to low morale and service disrupting industrial action.
- Service levels fall short - e.g. >7 million people on waiting lists for treatments
- Breakdowns frequently reported - such as the Infected Blood Scandal, failures in maternity treatment, etc.
- National health measures are lamentably low.
Reimagining healthcare requires a holistic systemic rethinking. It can’t be done piecemeal, and it cannot be undertaken by individuals who are blinkered by elements of the system ‘as is’ - not predisposed towards one or another set of potential outcomes. The process to arrive at a solution for healthcare in UK, that is future-relevant is disarmingly straight-forward, in equal measure to the complexity and opaqueness of whatever the eventual resulting reimagined system might be. And that’s the key point – no one can enter the process of reimagining the future of healthcare if they start with a position of advocacy for what the outcome may look like.
Twenty years ago, Singapore embarked on such a reimagining, and emerged successfully, with significant innovation and reorganisation. The reimagining process in Singapore, was jointly sponsored by the opposing sets of concerns and objectives of the Ministry of Health and the Ministry of Finance - united however in the recognition that a new financially sustainable way forward was required to improve the national health outcomes desired. To quote the Singapore Ministry of Health whose tag-line is ‘Achieving More with Less’:
“Unlike some countries……Singapore is achieving similar outcomes with less: Spending about 4% of our GDP annually on healthcare…..Yet our health outcomes are comparable with many developed countries. …..Spending more to achieve the same outcome is not a smart use of taxpayers’ money.”
However, it is not possible nor appropriate to look to any other country and seek to mimic the solution that they have adopted. Instead, we can look at the process that Singapore followed and see the transformative success that was achieved through creative thinking and the willingness of all parties to explore and redefine the possible.
Representatives from a very broad selection of stakeholders (community, government, providers of all types, insurance companies, research, public and private sector, academics, etc.) were invited to participate. Initially ‘everyone’ spoke passionately about their community, their entity, the outcomes that they wanted to see. People ‘dug in’ emotionally for a long campaign of arguing their case and hoping to sway the outcomes. The process would have stagnated but instead was reconceived.
- Firstly everyone who wanted to stay involved in the initiative needed to come to a common acceptance of what was unacceptable and unsustainable with the current situation, there had to be agreement to the minimum performance requirements for the future system (whatever that system may look like). This included requirements such as universal access for citizens, agreement on a sustainable level of state financial support (% of GDP), key metrics for the quality of care to be provided and the health metrics for the nation.
- Once that common-contract of objectives was established, multi-stakeholder taskforces were assembled to address each area that would cascade to the desired outcomes. The requirement for each taskforce being to come up with new ideas and structures, not to argue the pros and cons of the existing. Everyone had to pull together to pool ideas to find new ways forward.
A similar process is urgently needed to reimagine healthcare in the UK. Politicians may feel they are acting by ordering ‘another review of the NHS’ but that is an approach that has been tried several times before! A new approach is needed. A holistic reimagining of the entire HeathCare sector and policy framework – including what is the role of the NHS in the future. It needs to involve thousands of informed stakeholders. Participants in the process must free their minds from the existing structures and policies and instead come together to find innovative ways of achieving a commonly shared set of desired outcomes. We can expect that some elements that will need to be incorporated will include: a greater role for the private sector, greater personal responsibility and choice, universal access for an agreed scope of population, clarity on national health outcome objectives, the adoption of an objective and sustainable cap for public spending.
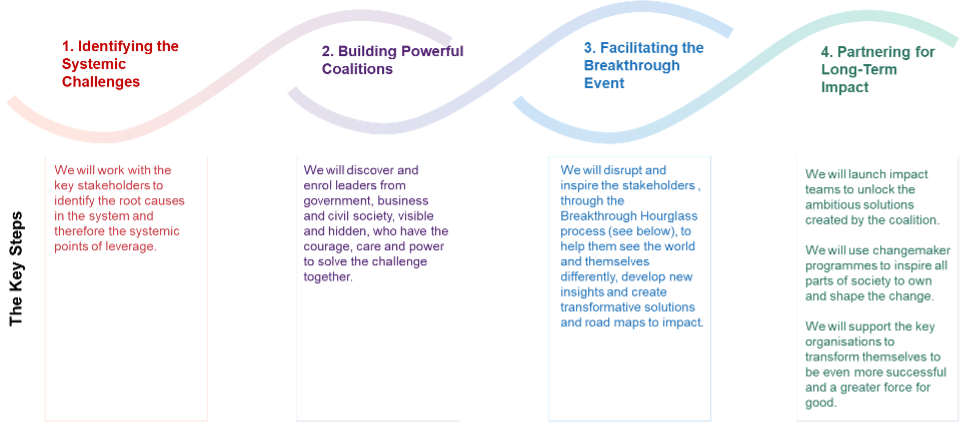
Systemic change is possible and the steps are known, but there has to be the willingness to create and sustain the process; governance and participants need to bring their insights but not be blinkered or biased. It is only by coming together through collaborative creative process that complex systems can be reimagined. The process has four stages as shown in the diagram below.
The Breakthrough Hourglass (shown below) is a problem-solving framework that has been evolved over many years of experience. It is a creative process that takes all the stakeholders on a journey of seeing things differently, surfacing new insights, and shaping the future together. It focuses on both solving the systemic challenges as well as societal leadership required. It has been applied successfully in contexts of conflict, combatting human trafficking, climate action and sustainable food.

Healthcare in the UK is in urgent need of being reimagined. Experience shows that there are only two ways to bring about systemic change at a national level. One is well- meaning and informed individuals coming together in a structured creative process that has senior-most level ownership and impartial governance. Where there is absolute clarity on the urgency and importance, a commitment to an integrated set of apparently conflicting goals and the obligation that participants are unbiased and unblinkered. The other path is gradual systemic failure and a catalysing external shock that then triggers a disaster recovery taskforce; but the risk then is there is still not the leadership to sponsor a holistic reimagination.
Thank you to Simon (Mac) McKenzie of the Bridge Institute for his collaboration and contribution to this blog post. Mac and the Bridge Institute apply these principles and approaches in a wide variety of contexts.
All articles posted on this blog give the views of the author(s), and not the position of the IPR, nor of the University of Bath.